Below are two detailed articles citing the documented true scientific fact that face masks cannot stop the spread of COVID-19 and actually spreads the virus. COVID-19 is nothing more than a politically motivated social engineering psychological operation. After all, what are the facts? Less than 1 percent of COVID-19 infections end in death. Not 3.5 to 5% as fear mongered. Another lie. Do you see the New World Order deindustrialization/collectivist pattern developing here? If not, please get your eyes examined. Or your head, repectfully.
There have been extensive randomized controlled trial (RCT) studies, and meta-analysis reviews of RCT studies, which all show that masks and respirators do not work to prevent respiratory influenza-like illnesses, or respiratory illnesses believed to be transmitted by droplets and aerosol particles.
Furthermore, the relevant known physics and biology, which I review, are such that masks and respirators should not work. It would be a paradox if masks and respirators worked, given what we know about viral respiratory diseases: The main transmission path is long-residence-time aerosol particles (< 2.5 μm), which are too fine to be blocked, and the minimum-infective dose is smaller than one aerosol particle.
The present paper about masks illustrates the degree to which governments, the mainstream media, and institutional propagandists can decide to operate in a science vacuum, or select only incomplete science that serves their interests. Such recklessness is also certainly the case with the current global lockdown of over 1 billion people, an unprecedented experiment in medical and political history.
Review of the Medical Literature Here are key anchor points to the extensive scientific literature that establishes that wearing surgical masks and respirators (e.g., “N95”) does not reduce the risk of contracting a verified illness:
Jacobs, J. L. et al. (2009) “Use of surgical face masks to reduce the incidence of the common cold among health care workers in Japan: A randomized controlled trial,” American Journal of Infection Control, Volume 37, Issue 5, 417 – 419. https://www.ncbi.nlm.nih.gov/pubmed/19216002
N95-masked health-care workers (HCW) were significantly more likely to experience headaches. Face mask use in HCW was not demonstrated to provide benefit in terms of cold symptoms or getting colds.
None of the studies reviewed showed a benefit from wearing a mask, in either HCW or community members in households (H). See summary Tables 1 and 2 therein.
“There were 17 eligible studies. … None of the studies established a conclusive relationship between mask/respirator use and protection against influenza infection.”
Smith, J.D. et al. (2016) “Effectiveness of N95 respirators versus surgical masks in protecting health care workers from acute respiratory infection: a systematic review and meta-analysis,” CMAJ Mar 2016 https://www.cmaj.ca/content/188/8/567
“We identified six clinical studies … . In the meta-analysis of the clinical studies, we found no significant difference between N95 respirators and surgical masks in associated risk of (a) laboratory-confirmed respiratory infection, (b) influenza-like illness, or (c) reported work-place absenteeism.”
Offeddu, V. et al. (2017) “Effectiveness of Masks and Respirators Against Respiratory Infections in Healthcare Workers: A Systematic Review and Meta-Analysis,” Clinical Infectious Diseases, Volume 65, Issue 11, 1 December 2017, Pages 1934–1942, https://academic.oup.com/cid/article/65/11/1934/4068747
“Self-reported assessment of clinical outcomes was prone to bias. Evidence of a protective effect of masks or respirators against verified respiratory infection (VRI) was not statistically significant”; as per Fig. 2c therein:
Radonovich, L.J. et al. (2019) “N95 Respirators vs Medical Masks for Preventing Influenza Among Health Care Personnel: A Randomized Clinical Trial,” JAMA. 2019; 322(9): 824–833. https://jamanetwork.com/journals/jama/fullarticle/2749214
“Among 2862 randomized participants, 2371 completed the study and accounted for 5180 HCW-seasons. ... Among outpatient health care personnel, N95 respirators vs medical masks as worn by participants in this trial resulted in no significant difference in the incidence of laboratory-confirmed influenza.”
“A total of six RCTs involving 9,171 participants were included. There were no statistically significant differences in preventing laboratory-confirmed influenza, laboratory-confirmed respiratory viral infections, laboratory-confirmed respiratory infection, and influenza-like illness using N95 respirators and surgical masks. Meta-analysis indicated a protective effect of N95 respirators against laboratory-confirmed bacterial colonization (RR = 0.58, 95% CI 0.43-0.78). The use of N95 respirators compared with surgical masks is not associated with a lower risk of laboratory-confirmed influenza.”
Conclusion Regarding That Masks Do Not Work No RCT study with verified outcome shows a benefit for HCW or community members in households to wearing a mask or respirator. There is no such study. There are no exceptions.
Likewise, no study exists that shows a benefit from a broad policy to wear masks in public (more on this below).
Furthermore, if there were any benefit to wearing a mask, because of the blocking power against droplets and aerosol particles, then there should be more benefit from wearing a respirator (N95) compared to a surgical mask, yet several large meta-analyses, and all the RCT, prove that there is no such relative benefit.
Masks and respirators do not work.
Precautionary Principle Turned on Its Head with Masks In light of the medical research, therefore, it is difficult to understand why public-health authorities are not consistently adamant about this established scientific result, since the distributed psychological, economic, and environmental harm from a broad recommendation to wear masks is significant, not to mention the unknown potential harm from concentration and distribution of pathogens on and from used masks. In this case, public authorities would be turning the precautionary principle on its head (see below).
Physics and Biology of Viral Respiratory Disease and of Why Masks Do Not Work In order to understand why masks cannot possibly work, we must review established knowledge about viral respiratory diseases, the mechanism of seasonal variation of excess deaths from pneumonia and influenza, the aerosol mechanism of infectious disease transmission, the physics and chemistry of aerosols, and the mechanism of the so-called minimum-infective-dose.
In addition to pandemics that can occur anytime, in the temperate latitudes there is an extra burden of respiratory-disease mortality that is seasonal, and that is caused by viruses. For example, see the review of influenza by Paules and Subbarao (2017). This has been known for a long time, and the seasonal pattern is exceedingly regular. (Publisher's note: All links to source references to studies here forward are found at the end of this article.)
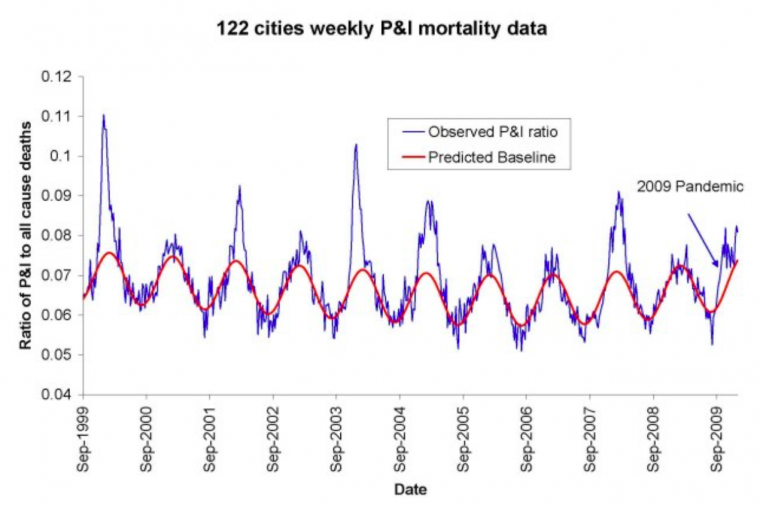
For example, see Figure 1 of Viboud (2010), which has “Weekly time series of the ratio of deaths from pneumonia and influenza to all deaths, based on the 122 cities surveillance in the US (blue line). The red line represents the expected baseline ratio in the absence of influenza activity,” here:
The seasonality of the phenomenon was largely not understood until a decade ago. Until recently, it was debated whether the pattern arose primarily because of seasonal change in virulence of the pathogens, or because of seasonal change in susceptibility of the host (such as from dry air causing tissue irritation, or diminished daylight causing vitamin deficiency or hormonal stress). For example, see Dowell (2001).
In a landmark study, Shaman et al. (2010) showed that the seasonal pattern of extra respiratory-disease mortality can be explained quantitatively on the sole basis of absolute humidity, and its direct controlling impact on transmission of airborne pathogens.
Lowen et al. (2007) demonstrated the phenomenon of humidity-dependent airborne-virus virulence in actual disease transmission between guinea pigs, and discussed potential underlying mechanisms for the measured controlling effect of humidity.
The underlying mechanism is that the pathogen-laden aerosol particles or droplets are neutralized within a half-life that monotonically and significantly decreases with increasing ambient humidity. This is based on the seminal work of Harper (1961). Harper experimentally showed that viral-pathogen-carrying droplets were inactivated within shorter and shorter times, as ambient humidity was increased.
Harper argued that the viruses themselves were made inoperative by the humidity (“viable decay”), however, he admitted that the effect could be from humidity-enhanced physical removal or sedimentation of the droplets (“physical loss”): “Aerosol viabilities reported in this paper are based on the ratio of virus titre to radioactive count in suspension and cloud samples, and can be criticized on the ground that test and tracer materials were not physically identical.”
The latter (“physical loss”) seems more plausible to me, since humidity would have a universal physical effect of causing particle/droplet growth and sedimentation, and all tested viral pathogens have essentially the same humidity-driven “decay.” Furthermore, it is difficult to understand how a virion (of all virus types) in a droplet would be molecularly or structurally attacked or damaged by an increase in ambient humidity. A “virion” is the complete, infective form of a virus outside a host cell, with a core of RNA or DNA and a capsid. The actual mechanism of such humidity-driven intra-droplet “viable decay” of a virion has not been explained or studied.
In any case, the explanation and model of Shaman et al. (2010) is not dependent on the particular mechanism of the humidity-driven decay of virions in aerosol/droplets. Shaman’s quantitatively demonstrated model of seasonal regional viral epidemiology is valid for either mechanism (or combination of mechanisms), whether “viable decay” or “physical loss.”
The breakthrough achieved by Shaman et al. is not merely some academic point. Rather, it has profound health-policy implications, which have been entirely ignored or overlooked in the current coronavirus pandemic.
In particular, Shaman’s work necessarily implies that, rather than being a fixed number (dependent solely on the spatial-temporal structure of social interactions in a completely susceptible population, and on the viral strain), the epidemic’s basic reproduction number (R0) is highly or predominantly dependent on ambient absolute humidity.
For a definition of R0, see HealthKnowlege-UK (2020): R0 is “the average number of secondary infections produced by a typical case of an infection in a population where everyone is susceptible.” The average R0 for influenza is said to be 1.28 (1.19–1.37); see the comprehensive review by Biggerstaff et al. (2014).
In fact, Shaman et al. showed that R0 must be understood to seasonally vary between humid-summer values of just larger than “1” and dry-winter values typically as large as “4” (for example, see their Table 2). In other words, the seasonal infectious viral respiratory diseases that plague temperate latitudes every year go from being intrinsically mildly contagious to virulently contagious, due simply to the bio-physical mode of transmission controlled by atmospheric humidity, irrespective of any other consideration.
Therefore, all the epidemiological mathematical modeling of the benefits of mediating policies (such as social distancing), which assumes humidity-independent R0 values, has a large likelihood of being of little value, on this basis alone. For studies about modeling and regarding mediation effects on the effective reproduction number, see Coburn (2009) and Tracht (2010).
To put it simply, the “second wave” of an epidemic is not a consequence of human sin regarding mask wearing and hand shaking. Rather, the “second wave” is an inescapable consequence of an air-dryness-driven many-fold increase in disease contagiousness, in a population that has not yet attained immunity.
If my view of the mechanism is correct (i.e., “physical loss”), then Shaman’s work further necessarily implies that the dryness-driven high transmissibility (large R0) arises from small aerosol particles fluidly suspended in the air; as opposed to large droplets that are quickly gravitationally removed from the air.
Such small aerosol particles fluidly suspended in air, of biological origin, are of every variety and are everywhere, including down to virion-sizes (Despres, 2012). It is not entirely unlikely that viruses can thereby be physically transported over inter-continental distances (e.g., Hammond, 1989).
More to the point, indoor airborne virus concentrations have been shown to exist (in day-care facilities, health centers, and on-board airplanes) primarily as aerosol particles of diameters smaller than 2.5 μm, such as in the work of Yang et al. (2011):
“Half of the 16 samples were positive, and their total virus −3 concentrations ranged from 5800 to 37 000 genome copies m . On average, 64 per cent of the viral genome copies were associated with fine particles smaller than 2.5 μm, which can remain suspended for hours. Modeling of virus concentrations indoors suggested a source strength of 1.6 ± 1.2 × 105 genome copies m−3 air h−1 and a deposition flux onto surfaces of 13 ± 7 genome copies m−2 h−1 by Brownian motion. Over one hour, the inhalation dose was estimated to be 30 ± 18 median tissue culture infectious dose (TCID50), adequate to induce infection. These results provide quantitative support for the idea that the aerosol route could be an important mode of influenza transmission.”
Such small particles (< 2.5 μm) are part of air fluidity, are not subject to gravitational sedimentation, and would not be stopped by long-range inertial impact. This means that the slightest (even momentary) facial misfit of a mask or respirator renders the design filtration norm of the mask or respirator entirely irrelevant. In any case, the filtration material itself of N95 (average pore size ~0.3−0.5 μm) does not block virion penetration, not to mention surgical masks. For example, see Balazy et al. (2006).
Mask stoppage efficiency and host inhalation are only half of the equation, however, because the minimal infective dose (MID) must also be considered. For example, if a large number of pathogen-laden particles must be delivered to the lung within a certain time for the illness to take hold, then partial blocking by any mask or cloth can be enough to make a significant difference.
On the other hand, if the MID is amply surpassed by the virions carried in a single aerosol particle able to evade mask-capture, then the mask is of no practical utility, which is the case.
Yezli and Otter (2011), in their review of the MID, point out relevant features:
Most respiratory viruses are as infective in humans as in tissue culture having optimal laboratory susceptibility
It is believed that a single virion can be enough to induce illness in the host
The 50-percent probability MID (“TCID50”) has variably been found to be in the range 100−1000 virions
There are typically 10 to 3rd power − 10 to 7th power virions per aerolized influenza droplet with diameter 1 μm − 10 μm
The 50-percent probability MID easily fits into a single (one) aerolized droplet
For further background:
A classic description of dose-response assessment is provided by Haas (1993).
Zwart et al. (2009) provided the first laboratory proof, in a virus-insect system, that the action of a single virion can be sufficient to cause disease.
Baccam et al. (2006) calculated from empirical data that, with influenza A in humans,“we estimate that after a delay of ~6 h, infected cells begin producing influenza virus and continue to do so for ~5 h. The average lifetime of infected cells is ~11 h, and the half-life of free infectious virus is ~3 h. We calculated the [in-body] basic reproductive number, R0, which indicated that a single infected cell could produce ~22 new productive infections.”
Brooke et al. (2013) showed that, contrary to prior modeling assumptions, although not all influenza-A-infected cells in the human body produce infectious progeny (virions), nonetheless, 90 percent of infected cell are significantly impacted, rather than simply surviving unharmed.
All of this to say that: if anything gets through (and it always does, irrespective of the mask), then you are going to be infected. Masks cannot possibly work. It is not surprising, therefore, that no bias-free study has ever found a benefit from wearing a mask or respirator in this application.
Therefore, the studies that show partial stopping power of masks, or that show that masks can capture many large droplets produced by a sneezing or coughing mask-wearer, in light of the above-described features of the problem, are irrelevant. For example, such studies as these: Leung (2020), Davies (2013), Lai (2012), and Sande (2008).
Why There Can Never Be an Empirical Test of a Nation-Wide Mask-Wearing Policy As mentioned above, no study exists that shows a benefit from a broad policy to wear masks in public. There is good reason for this. It would be impossible to obtain unambiguous and bias-free results [because]:
Any benefit from mask-wearing would have to be a small effect, since undetected in controlled experiments, which would be swamped by the larger effects, notably the large effect from changing atmospheric humidity.
Mask compliance and mask adjustment habits would be unknown.
Mask-wearing is associated (correlated) with several other health behaviors; see Wada (2012).
The results would not be transferable, because of differing cultural habits.
Compliance is achieved by fear, and individuals can habituate to fear-based propaganda, and can have disparate basic responses.
Monitoring and compliance measurement are near-impossible, and subject to large errors.
Self-reporting (such as in surveys) is notoriously biased, because individuals have the self-interested belief that their efforts are useful.
Progression of the epidemic is not verified with reliable tests on large population samples, and generally relies on non-representative hospital visits or admissions.
Several different pathogens (viruses and strains of viruses) causing respiratory illness generally act together, in the same population and/or in individuals, and are not resolved, while having different epidemiological characteristics.
Unknown Aspects of Mask Wearing Many potential harms may arise from broad public policies to wear masks, and the following unanswered questions arise:
Do used and loaded masks become sources of enhanced transmission, for the wearer and others?
Do masks become collectors and retainers of pathogens that the mask wearer would otherwise avoid when breathing without a mask?
Are large droplets captured by a mask atomized or aerolized into breathable components? Can virions escape an evaporating droplet stuck to a mask fiber?
What are the dangers of bacterial growth on a used and loaded mask?
How do pathogen-laden droplets interact with environmental dust and aerosols captured on the mask?
What are long-term health effects on HCW, such as headaches, arising from impeded breathing?
Are there negative social consequences to a masked society?
Are there negative psychological consequences to wearing a mask, as a fear-based behavioral modification?
What are the environmental consequences of mask manufacturing and disposal?
Do the masks shed fibers or substances that are harmful when inhaled?
Conclusion By making mask-wearing recommendations and policies for the general public, or by expressly condoning the practice, governments have both ignored the scientific evidence and done the opposite of following the precautionary principle.
In an absence of knowledge, governments should not make policies that have a hypothetical potential to cause harm. The government has an onus barrier before it instigates a broad social-engineering intervention, or allows corporations to exploit fear-based sentiments.
Furthermore, individuals should know that there is no known benefit arising from wearing a mask in a viral respiratory illness epidemic, and that scientific studies have shown that any benefit must be residually small, compared to other and determinative factors.
Otherwise, what is the point of publicly funded science?
The present paper about masks illustrates the degree to which governments, the mainstream media, and institutional propagandists can decide to operate in a science vacuum, or select only incomplete science that serves their interests. Such recklessness is also certainly the case with the current global lockdown of over 1 billion people, an unprecedented experiment in medical and political history.
Denis G. Rancourt is a researcher at the Ontario Civil Liberties Association (OCLA.ca) and is formerly a tenured professor at the University of Ottawa, Canada. This paper was originally published at Rancourt's account on ResearchGate.net. As of June 5, 2020, this paper was removed from his profile by its administrators at Researchgate.net/profile/D_Rancourt. At Rancourt's blog ActivistTeacher.blogspot.com,he recounts the notification and responses he received from ResearchGate.net and states, “This is censorship of my scientific work like I have never experienced before.”
The original April 2020 white paper in .pdf format is available here, complete with charts that have not been reprinted in the Reader print or web versions.
Endnotes: Baccam, P. et al. (2006) “Kinetics of Influenza A Virus Infection in Humans”, Journal of Virology Jul 2006, 80 (15) 7590-7599; DOI: 10.1128/JVI.01623-05 https://jvi.asm.org/content/80/15/7590
Balazy et al. (2006) “Do N95 respirators provide 95% protection level against airborne viruses, and how adequate are surgical masks?”, American Journal of Infection Control, Volume 34, Issue 2, March 2006, Pages 51-57. doi:10.1016/j.ajic.2005.08.018 http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.488.4644&rep=rep1&type=pdf
Biggerstaff, M. et al. (2014) “Estimates of the reproduction number for seasonal, pandemic, and zoonotic influenza: a systematic review of the literature”, BMC Infect Dis 14, 480 (2014). https://doi.org/10.1186/1471-2334-14-480
Brooke, C. B. et al. (2013) “Most Influenza A Virions Fail To Express at Least One Essential Viral Protein”, Journal of Virology Feb 2013, 87 (6) 3155-3162; DOI: 10.1128/JVI.02284-12 https://jvi.asm.org/content/87/6/3155
Coburn, B. J. et al. (2009) “Modeling influenza epidemics and pandemics: insights into the future of swine flu (H1N1)”, BMC Med 7, 30. https://doi.org/10.1186/1741-7015-7-30
Davies, A. et al. (2013) “Testing the Efficacy of Homemade Masks: Would They Protect in an Influenza Pandemic?”, Disaster Medicine and Public Health Preparedness, Available on CJO 2013 doi:10.1017/dmp.2013.43 http://journals.cambridge.org/abstract_S1935789313000438
Despres, V. R. et al. (2012) “Primary biological aerosol particles in the atmosphere: a review”, Tellus B: Chemical and Physical Meteorology, 64:1, 15598, DOI: 10.3402/tellusb.v64i0.15598 https://doi.org/10.3402/tellusb.v64i0.15598
Dowell, S. F. (2001) “Seasonal variation in host susceptibility and cycles of certain infectious diseases”, Emerg Infect Dis. 2001;7(3):369–374. doi:10.3201/eid0703.010301 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2631809/
Hammond, G. W. et al. (1989) “Impact of Atmospheric Dispersion and Transport of Viral Aerosols on the Epidemiology of Influenza”, Reviews of Infectious Diseases, Volume 11, Issue 3, May 1989, Pages 494–497, https://doi.org/10.1093/clinids/11.3.494
HealthKnowlege-UK (2020) “Charter 1a - Epidemiology: Epidemic theory (effective & basic reproduction numbers, epidemic thresholds) & techniques for analysis of infectious disease data (construction & use of epidemic curves, generation numbers, exceptional reporting & identification of significant clusters)”, HealthKnowledge.org.uk, accessed on 2020-04-10. https://www.healthknowledge.org.uk/public-health-textbook/research-methods/1a- epidemiology/epidemic-theory
Lai, A. C. K. et al. (2012) “Effectiveness of facemasks to reduce exposure hazards for airborne infections among general populations”, J. R. Soc. Interface. 9938–948 http://doi.org/10.1098/rsif.2011.0537
Leung, N.H.L. et al. (2020) “Respiratory virus shedding in exhaled breath and efficacy of face masks”, Nature Medicine (2020). https://doi.org/10.1038/s41591-020-0843-2
Lowen, A. C. et al. (2007) “Influenza Virus Transmission Is Dependent on Relative Humidity and Temperature”, PLoS Pathog 3(10): e151. https://doi.org/10.1371/journal.ppat.0030151
Sande, van der, M. et al. (2008) “Professional and Home-Made Face Masks Reduce Exposure to Respiratory Infections among the General Population”, PLoS ONE 3(7): e2618. doi:10.1371/journal.pone.0002618 https://doi.org/10.1371/journal.pone.0002618
Shaman, J. et al. (2010) “Absolute Humidity and the Seasonal Onset of Influenza in the Continental United States”, PLoS Biol 8(2): e1000316. https://doi.org/10.1371/journal.pbio.1000316
Tracht, S. M. et al. (2010) “Mathematical Modeling of the Effectiveness of Facemasks in Reducing the Spread of Novel Influenza A (H1N1)”, PLoS ONE 5(2): e9018. doi:10.1371/journal.pone.0009018 https://doi.org/10.1371/journal.pone.0009018
Viboud C. et al. (2010) “Preliminary Estimates of Mortality and Years of Life Lost Associated with the 2009 A/H1N1 Pandemic in the US and Comparison with Past Influenza Seasons”, PLoS Curr. 2010; 2:RRN1153. Published 2010 Mar 20. doi:10.1371/currents.rrn1153 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2843747/
Wada, K. et al. (2012) “Wearing face masks in public during the influenza season may reflect other positive hygiene practices in Japan”, BMC Public Health 12, 1065 (2012). https://doi.org/10.1186/1471-2458-12-1065
Yang, W. et al. (2011) “Concentrations and size distributions of airborne influenza A viruses measured indoors at a health centre, a day-care centre and on aeroplanes”, Journal of the Royal Society, Interface. 2011 Aug;8(61):1176-1184. DOI: 10.1098/rsif.2010.0686. https://royalsocietypublishing.org/doi/10.1098/rsif.2010.0686
Yezli, S., Otter, J.A. (2011) “Minimum Infective Dose of the Major Human Respiratory and Enteric Viruses Transmitted Through Food and the Environment”, Food Environ Virol 3, 1–30. https://doi.org/10.1007/s12560-011-9056-7
Zwart, M. P. et al. (2009) “An experimental test of the independent action hypothesis in virus– insect pathosystems”, Proc. R. Soc. B. 2762233–2242 http://doi.org/10.1098/rspb.2009.0064
Lisa Brosseau, ScD: "What we’re seeing is a lot of magical thinking. A lot of wishful thinking. Cloth masks are wishful thinking."
Lisa Brosseau, ScD, is a nationally recognized expert on infectious diseases. Brousseau taught for many years at the University of Illinois at Chicago. She may be retired from the university, but she’s not retired from teaching. She recently cowrote an opinion piece that drew a lot of notice: In it Brousseau argues that cloth masks offer no protection from COVID-19. As one might imagine, it drew a lot of attention and caused a fair amount of controversy. She recently sat down with Infection Control Today®to talk about her strong feelings about cloth masks and that data she used to reach her conclusions.
Infection Control Today®: What made you decide to write the piece?
Lisa Brosseau: The article started out with the goal of trying to look at the literature related to cloth masks in healthcare. And then it got expanded way beyond that to cloth masks and surgical masks and respirators for healthcare and for the community. It was much more comprehensive than I expected it to be. Took me a little longer to write but at the end of the day, I was looking at cloth masks and surgical masks and respirators from several points of view. First of all, for healthcare and community, but also do they work as source control? Or do they work as personal protective equipment? Or both? And at the end of the day, cloth masks in my opinion don’t work in any form. They aren’t very good at source control, except for maybe very large particles. And they should not be used in healthcare settings for a number of reasons. Surgical masks, I decided, based on the literature, might have a role as source control for people who have symptoms. Say if they’re staying home and they have some symptoms. They shouldn’t be something you’d wear if you have symptoms going out into the public because you shouldn’t be going out into the public service. But it’s a good option for patients to wear in healthcare settings where they-especially for those who are experiencing symptoms-to what I would call diminish the viral load. Basically, decrease the amount of particles, infectious particles in the air in a healthcare setting. So, at the end of the day, the only thing that provides personal protection for the person wearing the mask is a respirator. And that is the thing that healthcare workers should be wearing. Particularly if we’re worried about the small aerosols, small particles that people will generate when they’re infectious. And in fact, people generate particles, whether they’re infectious or not. But particularly when they’re infected and infectious, that will be present in the vicinity of a patient. The best protection in that case is for the healthcare worker to wear a respirator. And I’ve got asked a little bit to think about respirators for the community. You know, if we had a lot of respirators, that might be a good idea, but we don’t have very many of them. And so, for the purposes of saving those respirators for the people who really need them, I recommended that the public not be wearing respirators and not be buying respirators. And if they had them, please donate them even to healthcare workers. That’s a good summary.
ICT®: You did a deep dive into the literature. I saw you had many, many references. So, the mystery to me is why did the CDC say to people go out and wear cloth masks if you want to?
Brosseau: What’s interesting to me is if you look at the references that were listed on under their recommendation, none of them have anything to do with masks or the performance of masks or the performance of their filters or any of that. They’re all references related to pre-symptomatic or asymptomatic transmission. I didn’t get the message there entirely, but I was glad to see is that they recognized that asymptomatic and pre-symptomatic transmission are happening. My message would have been if those were the references I was looking at, is maybe we should actually be encouraging people to stay home more. My biggest problem with telling people they can wear masks is it gives you this false sense of security. And it might even encourage you to think that now you’re protected and you’re protecting people around you. My husband and I try to take a walk every afternoon, just to get out, get a little bit of fresh air and exercise. And I’m seeing more and more people now wearing cloth masks on the streets. And I don’t go to stores anymore, but my understanding is they’re wearing them there as well. I don’t have a problem with people wearing them. I just want them to understand that they aren’t very much more protective than if they weren’t wearing them. And they’re really not doing a whole lot of good for the people around them. So, we should continue to do social distancing as much as we possibly can. I have places that are saying that you actually have to wear them. New York where you’re supposed to wear them anytime you’re in contact with people. I don’t know. I just think it’s not recognizing that the mode of transmission for this organism is likely small aerosols and close range and wearing a cloth mask shouldn’t give you any feeling of safety for being close to people. It shouldn’t make you feel that you’re not generating small particles because you still are. And since we none of us know if we’re infected or infectious, many of us probably are and aren’t going to have symptoms because we know that that’s the case for at least some fraction of the population that we’re putting everyone around us at risk. And especially the people I most care about are the workers. Our essential workers are really key to our success in flattening the curve. And they’re the ones who make it possible for us to stay home and be isolated those of us who are privileged enough to have that opportunity. But we go out and think that we are doing something good for the public and the workers, and we’re actually not. I think we put them at more risk. So, I don’t understand the CDC’s recommendations for this. My guess is that there’s a lot of political pressure. And no government agency is entirely immune from political pressure. There’s pressure to open, right? There’s pressure to restart the economy. I understand that entirely. And so I think the feeling was, probably if we give everybody a mask, we can just reopen and everything’s going to be fine. I think we’re going to be shocked to find that that’s not going to work. And I mean, I won’t be shocked, but there will be lots of people who will be shocked. And in fact, I read an article recently about a funeral. A number of people who attended the funeral. They were all wearing masks. They were taking photos next to each other. They were talking and a number of people got infected. So, it’s very clear these things do no good.
ICT®: Have you gotten much feedback from healthcare workers or healthcare experts themselves?
Brosseau: Oh, yeah. There are a number who don’t agree, but there are a lot of people who didn’t agree with my first article about aerosol transmission either. I’m sort of used to it. The important thing is to say, here’s what the science tells us. My conversations with people these days, I often point out that what we’re seeing is a lot of magical thinking. A lot of wishful thinking. Cloth masks are wishful thinking. And people saying, well, they worked in Asia. There’s no evidence that they worked in Asia. In fact, it’s very clear that the healthcare workers in China, they may have been wearing cloth masks to start with, but when you look at pictures of what they were wearing later, they were wearing respirators. They were wearing full face gear and body gear and gloves. It was clear that even surgical masks weren’t working in healthcare settings or controlling COVID-19. I don’t understand it. The Asian countries wear masks for societal and cultural reasons, not because they actually think they’re protecting. I’m not an expert in epidemiology. So, I will leave the modeling to the to those who know more about how this is going to work, but I do know my history. And if you read about the 1918 influenza and the pandemic, it took almost two years for that to be completely done with. They did a lot of similar things. They closed down. They opened again. Then they had to close down and then they had to open again. Now, granted, they didn’t have a lot of what we have today. But in some ways, we’re not all that different from 1918. We don’t have any testing. We don’t have any contact tracing. They didn’t either. They didn’t even really know about that. They didn’t know much about viruses. So, we have huge amounts of scientific information. But we have almost no infrastructure anymore in public health. Without our infrastructure in public health and our resources to do contact tracing and testing…. And testing, I mean with tests that really work that are both highly specific and highly sensitive. And we don’t have any of those yet. In many ways we’re being forced to make many of the same decisions that were made during the 1918 influenza pandemic. And the results are going to be similar. We are trying to decide when to open it back up. No one really knows the perfect answer to that. The models, they’re not perfect, right? I know infection preventionists are often pulled in two directions. One is they have to worry about patients. The other is they have to worry about workers. And sometimes the things you do for patients don’t work for workers and sometimes the other way around. That’s why I recommend including your health and safety people, industrial hygienists, and others, because they can give you that perspective about workers that will help you make good decisions for both. And really, it should be a hand-in-hand decision making that goes on.
ICT®: Any final words about cloth masks?
Brosseau: I would really strongly encourage hospitals to stop asking people to send them cloth masks and instead asked for respirators. I don’t necessarily discourage the public from wearing them if it makes them feel comfortable, but I hope they don’t think that they’re protecting themselves.
This interview has been edited for clarity and length.
By Howard Nemaizer Welcome to the "new normal" New World Order.
Many sacrifices have been made because of the World Health Organization’s mandates to keep us safe from the COVID-19 “pandemic” hoax. 24/7 fear mongering propaganda and new normal social control have taken their toll on us all. From the start the W.H.O. data models and predictions were so far off, (like political polls), their reliability is questionable to say the least and criminal to say the most.
The COVID hoax revealed itself as clear as day recently when stringent authoritarian precautions limiting the freedom of all Americans was cast aside in the winds of social justice. It appears nationwide protests, violence, looting and rioting in the wake of yet another black man killed by a police officer is not a threat to our health, but going to religious services or funerals is. Unless your funeral was used to further propagandize a distraction agenda that has ignored the real serious issues in the black community; fatherless homes, abortion and black on black violence for decades. After all, keeping these atrocities going has buttered the exploitive race baiting bread of Al Sharpton and his ilk for 40 years.
Anyone remember Tawana Brawley?
After the horrific murder of George Floyd, tortured and asphyxiated by a psycho cop with a long history of complaints, the mass media agenda shift was so swift it was stunning. Hopefully, this tragic, sickening and sadistic murder will finally put a stop to police brutality. Certainly defunding the police is not a way to achieve this. It is however, a way to create further chaos. Now we have war lords armed with AR-15’s replacing police in Seattle, Washington and the mayor is ok with it. What madness…
In an instant, the media flipped 180 degrees from 24/7 COVID-19 propaganda to 24/7 propagandizing and martyring yet another “honest”, “good man”. In this case, the martyred gentle giant also happened to be a violent felon named, George Floyd. Mention this fact and you are labeled a racist. This use of undeserving martyrdom is an old school Stalinist communist tactic. Textbook.
As a result of the new aspect of this psyop, guilt plagued whites are now kneeling and kissing black people’s feet to make amends for their white privilege. It is truly incredible how much critical theory, the Frankfurt School of Thought, Gramschi socialism and other communist theories funded by the Ford, Carnegie and Rockefeller Foundations since 1908 have taken hold of many American’s psyche. We have forgotten who we are and where we come from. And many are taking our freedom for granted. Freedom is not free. Liberty requires eternal vigilance.
Society has conditioned many to believe that we should feel guilty for our past rather than proud. As if the Soviet Union, China, North Korea or any communist country offer a better way of life through social justice and equality rather than freedom and prosperity. Equality, like utopia are impossible dreams. But very alluring concepts.
The fact is, communism always leads to misery. But today’s communists, like those in the past falsely believe that it will be their generation that will be different. even though the fact that doing the same thing and expecting a different result is the very definition of insanity. I guess that is why communists will never learn. They are insane.
This current new George Floyd social justice aspect of the order out of chaos agenda was allowed to fester for weeks before the collectivists at the World Health Organization made even a peep about the dangers of such mass gatherings, let alone the deadly chaos, riots, looting and cop killing that has been mostly ignored by the mainstream media. But, to its totalitarian credit, the United Nations did call for a global police force to deal with future riots in the US. How nice of them, right?
This is the new normal. The new psyop. What’s next?
Back in January, 2020 Dr. Deception, Anthony Fauci told Americans that masks would not be needed to stop the spread of COVID-19, in fact that masks would not help stop the spread of COVID-19 and only the infected should wear masks. Fauci did however emphasize to the younger generation that it was A-OK to hook up and have all the sex they want, just to use condoms. Complete with a depopulation agenda plug. How nice, right?
In February, we were told that asymptomatic people could spread the virus and everyone must wear a mask and social distance, even though masks do nothing to actually stop the spread of the virus. They are great for social conditioning, however.
By March, 60% of America’s economy was shut down in fear of the spread of the virus. All of this, mandated by the World Health Organization (WHO), a United Nations Organization whose lack of transparency has scammed the world with false data and overstated gloom and doom predictions.
As result of all of this, the world economy is in chaos and free fall. Debt and unemployment is rising. Markets are unstable and lowering as the lies continue. The new propaganda pitch is that there will be a resurgence of COVID-19 in the fall. The problem is, markets believe the lies and react to them. For instance, in June 2019 the WHO ruled that, although the Ebola outbreak in the Congo was “a severe emergency,” it did not yet qualify as a global emergency. This was the second time the U.N. agency had decided that the Congo outbreak did not qualify to be a global emergency.
Then there is H1N1. “In the months leading up to the WHO’s declaration of the pandemic as a ‘level 6’ contagion which is the highest level, many countries including Germany, France, Italy and the UK made secret agreements with pharmaceutical companies. How nice, right?
These contracts obliged the countries to buy Swine Flu vaccinations only if the WHO raised the pandemic to a level 6.” The 2018 documentary TRUST WHO, filmmaker Lillian Franck exposed footage that revealed WHO delegates six weeks before the level 6 pandemic was issued describing swine Flu as a ‘moderate’ situation. Still a pandemic was announced. Why? As with the COVID-19 “pandemic” and all things New World Order, follow the money.
Remember we are dealing with communists, whose stated goal is the destruction of the middle class and private property. The lockdown has sucessfully permanently closed approximately 30% of private small businesses in the US. Millions of people have lost their jobs. Qui bono? Who benefits? Communists. By the WHO’s own admission, COVID-19 was declared a pandemic in order to avoid becoming a pandemic. For what purpose? To destroy the world’s economy to avoid a pandemic? Oh no! Henny Penny! Henny Penny! The sky is falling!
The best way to understand what it happening in America and the world today is to take a look at the past. After all, “Those who forget the past are condemned to repeat it”. – George Santayana
The past repeats. But it doesn’t repeat organically. The past is used to control the future. Erasing the past, history and monuments allows future rulers and tyrants to execute actions and atrocities again and again without recourse or understanding by the masses because they are ignorant of the true history. History divided into exoteric and esoteric interpretations. Hidden, so the rulers, adepts and initiates can continue to maintain power no matter who holds a high position in society or political office.
After World War I, the generational power elite conspirators failed in their attempt for world government with the League of Nations. As is now, the 1814-15 Congress of Vienna was designed to maintain the elite’s status quo and redesign Europe after the downfall of Napoleon. (Sound familiar? Echoes of World War 2)
The objective of the Congress of Vienna was to provide a long-term peace for Europe and setting the stage for world government. The goal was to restore old borders but to resize the main powers so they could balance each other and remain at peace while suppressing the rise of liberty and freedom among the masses to benefit the monarch and uber elite classes. Although there have been some variations, this augmentation exists to this very day. This is what they are still striving for. The Great Work. And it is the Great Utopian Lie.
The fact is, the so called “war to end all wars” had no just cause other than to fund a war machine, consolidate economic power and create billions in profits for American bankers. Bankers who funded both sides of the World War 1, the Bolshevik Revolution, the rise of Hitler and every war since, thanks to the creation of the Federal Reserve crime syndicate in 1913. The horrors of World War 1 were used as a pretext for the creation of the League Of Nations. The league failed because individual nations would lose too much of their sovereignty by joining. Unfortunately, America has experienced a slow and steady dissolution of sovereignty since the creation of the United Nations by communist spies such as Alger Hiss and others who worked and are still working to complete the Great Work, the creation of a totalitarian socialist world government.
Ever since World War 1, the ruling class and thier elitist minions inundated the American people with world government globalist propaganda through conspiratorial organizations like the Council on Foreign Relations (CFR), founded in 1919 in Paris and headquartered in New York City in 1921. The CFR was influential and successful in aligning the United States into the United Nations after World War II.
During the 1950’s the Reese Committee investigated the Rockefeller, Carnegie and Ford foundations, but as the the investigation opened a treasonous can of worms, it was quickly squashed by the Anglo-American world government establishment.
During the investigation Rowan Gaither, President of the Ford Foundation admited to congressional examiner Norman Dodd that the goals of the Ford Foundation was to “fundamentally change the teaching of American History by issuing grants to colleges, universities and professors that pledged to hire professors and administrators recommended by the Foundation.
This was done so as to bring about “a change in American society where it could be comfortably merged with the Soviet Union.” WATCH VIDEO BELOW:
Norman Dodd interview with G. Edward Griffin (1984)
For generations we have seen the elite’s compulsive goal for world government. More and more, their zealous authoritarian lust for power is right out in the open. Our leaders lie, cheat and steal, but we still believe and follow their recommendations. Time and time again. And more times than not, the results are not good.
The hidden masters operating behind the scenes tricked us into both world wars to consolidate and collectivize their power. As at the end of the Napoleonic Wars, the end of World War 1, and War 2, the banking and power elite who operate in secret have once again chipped away at the stone of liberty in hopes of creating their New World Order.
Here is further insight from Georgetown Professor Carroll Quigley, who spent 2 years researching records at the Council on Foreign Relations to write his book, Tragedy And Hope”.
“The argument that the two parties should represent opposed ideals and policies, one, perhaps, of the Right and the other of the Left, is a foolish idea acceptable only to doctrinaire and academic thinkers. Instead, the two parties should be almost identical, so that the American people can ‘throw the rascals out’ at any election without leading to any profound or extensive shifts in policy” (Georgetown University Professor Carroll Quigley, Tragedy and Hope, 1966.)
“The powers of financial capitalism had another far-reaching aim, nothing less than to create a world system of financial control in private hands able to dominate the political system of each country and the economy of the world as a whole. This system was to be controlled in a feudalist fashion by the central banks of the world acting in concert, by secret agreements arrived at in frequent private meetings and conferences.” (Georgetown University Professor Carroll Quigley, Tragedy and Hope, p. 324. 1966.)
“There does exist, and has existed for a generation, an international Anglophile network which operates, to some extent, in the way the radical Right believes the Communists act. In fact, this network, which we may identify as the Round Table Groups, has no aversion to cooperating with the Communists, or any other groups, and frequently does so. I know of the operations of this network because I have studied it for twenty years and was permitted for two years, in the early 1960’s, to examine its papers and secret records. I have no aversion to it or to most of its instruments. I have objected, both in the past and recently, to a few of its policies, but in general my chief difference of opinion is that it wishes to remain unknown, and I believe its role in history is significant enough to be known.” (Georgetown University Professor Carroll Quigley, Tragedy & Hope: A History of the World in Our Time, p. 950. 1964.)
“The Council on Foreign Relations is the American branch of a society which originated in England [and] believes national boundaries should be obliterated and one-world rule established.” (Georgetown University Professor Carroll Quigley, Tragedy and Hope, A History of the World in Our Time, p. 951. 1966.)
This should all start to make sense. As we see the apparent love affair with China and the World Health Organization, it simply stands to reason that birds of a feather flock together. The entire COVID-19 hoax clearly amplifies all of this.
Is it a coincidence that the United States worker has been eviscerated by death from a 1,000 cuts of globalism, NAFTA, GATT and the revised World Trade Organization? Is it a coincidence that manufacturing shifted to China? Is it a coincidence that America is bashed by the controlled mainstream media, but China’s human right abuses are ignored?
How has all of this happened? Well, the United Nations was conceived by elitists forwarding and profiting from communism. It has always been run by Communists for Communist purposes and to serve the interests of the elite at the top of the pyramid. Founded at the San Francisco Conference in 1945 as the war was coming to an end, the United Nations first Secretary-General at the UN was Alger Hiss.
Alger Hiss
Hiss, one of the drafters of the United Nations charter, was a charmingly handsome communist, who was given the Edward Burnaysian propaganda spin complete with a Madison Avenue shine, gracing all the long standing insider New World Order publications like TIME, LIFE and Newsweek.
Hiss was also the Director of the State Department’s Office of Special Political Affairs which allowed him to appoint all the members of the U.S. UN delegation. In February, 1945, much of the ground work for the UN was arranged and layed out at Yalta, in the Soviet Union, where central Europe was secretly deeded to Stalin and the Iron Curtain was born. So was the term, the Cold War, as coined by celebrated communist propagandist Walter Lippmann.
Hiss of course was later exposed as a Soviet spy and convicted and imprisoned for lying under oath about his Communist activities. In 1946 at the first London Conference, Hiss arranged for the Soviets to run UN military activities and for the United States to run UN financial activities, which meant in effect that the Soviet Union won the right to run the UN and the US won the right to pay for it.
Congressman Larry Mc Donald exposes CFR/State Department agenda for world government.
To further communist activities at the time, in the May/June issue of the Partisan Review in 1947, Arthur Schlessinger candidly admitted that America’s secret agenda was to adopt socialism, but that the American people were not “sophisticated enough to see the value of socialism” so this agenda would continue under the guise of maintaining peace in the world, while both waging war and forwarding communism. It is important to note that Alger Hiss was just one of many pro-Soviet/UN/globalist scum who betrayed America at that time. J.D. Rockefeller, Prescott Bush, Armond Hammer and George Marshall to name just a few. ROckefeller donated the land where the United Nations building stands to this day in New York City.
The fact is, there are far too many subversive traitors, operatives and pirates to list in this article from both sides of the political spectrum, both past and present. From George HW Bush to Bill Clinton to GW Bush to Obama. But Americans are not “sophisticated enough” to see this false Left/Right paradigm being used to forward collectivist world government. Remember, so called Republican conservative GW Bush called for an ever-stronger UN, a UN with “spine,” a UN with “backbone,” a UN determined to avoid the fate of the League of Nations.
Remember that the purpose of all this was and remains the creation of a totalitarian socialist world government, in which our own U.S. government would at first be subservient and later dissolved. This objective is always being forwarded by execution actions and congressional legislation, or lack of it.
The mayhem and insanity we see in our streets today is a good example of just how well this phase of the New World Order is escalating, but the roots lay far in the past.
In the 1968 book, The Actor (Boston, Western Islands), the following statement can be found published by Foreign Affairs, the monthly periodical of the Council on Foreign Relations. John Foster Dulles, the Marxist revolutionary who was Eisenhower’s Secretary of State and co-founding head of the CIA, talks about UN legislation
“. . . The achievement of such a body of laws calls for a lawmaking process. And to enforce them there is required a judicial system and police force. . . “So far, we haven’t been able to arrange this,” Dulles complains. But then he adds, “We must not accept that condition as permanent. . . .”
This agenda for a world legislature, judiciary and military adds up to a government. Recent calls for a National police force and the dismantling of local police departments is yet another clear example of this ploy working to disrupt society into chaos and have the United Nations come in as the savior. Proof of this ongoing reality isn’t hard to find. In September, 1961, United States State Department Publication 7277, entitled “Freedom From War, The United States Program for General and Complete Disarmament in a Peaceful World” remains official U.S. government policy. Here is an excerpt from the document:
“The disbanding of all national armed forces and the prohibition of their reestablishment in any form whatsoever other than those required to preserve internal order. . .”
If you are worried about police departments being eliminated, just wait — Official U.S. government policy is to eliminate all militaries, including our own. Remember when Obama decimated Our military as the United Nations increased its own military?
The United Nations Peace Force. A one world army patterned to keep the status quo in power. A one world totalitarian socialist state where the political and economic systems of every country on earth is “controlled by the central bankers of the world working in concert in a fuedalist fashion,” as quoted by Carroll Quigley in his 1966 book, “Tragedy And Hope: A History of the World In Our Time”, (this and links to all books mentioned in this article are available at HowardNema.com).
The 1961 “Freedom From War, The United States Program for General and Complete Disarmament in a Peaceful World” documents further states:
“. . . In Stage III progressive controlled disarmament and continuously developing principles and procedures of international law would proceed to a point where no state would have the military power to challenge the progressively strengthened U.N. Peace Force. . .”
This means when the process is complete, America and the entire world would be completely defenseless. There would be no military other than the UN Peace Force. Can we all see where this war on the police is heading? Can we see the writing on the wall?
The UN was conceived by Communists, founded by Communists and always has been run by Communists for Communist purposes. This eventually means the complete Communist subjugation of the United States. And as we are all witnessing, is happening before our very eyes in the streets of Minneapolis, Seattle and other leftist/democrat run cities and states across the country.
As mentioned, the New World Order operators are bi-partisan. After years of being out of UNESCO, George Bush adopted the program, whose protocols have flooded the nation’s schools with Communist world government propaganda ever since and continues to do so. After all, that was its main purposes.
Along these lines, UNICEF, the UN Children’s Fund pushes child sex with homosexuals and with animals. In South Africa, a UNICEF outfit called LoveLife promotes sodomy and abortion. The UN also wants bugs to be added to our diets and to eliminate meat eating.
If that isn’t bad enough, the June 24th, 1997 Village Voice reported on sexual exploitation, torture and murder of children, by UN “Peacekeeping” soldiers, including photos of UN “peace keepers” burning a living child. This story should have been on the front page of every newspaper in the United States. Have you ever even heard about it? I bet not.
 Masks and respirators do not work.
There have been extensive randomized controlled trial (RCT) studies, and meta-analysis reviews of RCT studies, which all show that masks and respirators do not work to prevent respiratory influenza-like illnesses, or respiratory illnesses believed to be transmitted by droplets and aerosol particles.
Furthermore, the relevant known physics and biology, which I review, are such that masks and respirators should not work. It would be a paradox if masks and respirators worked, given what we know about viral respiratory diseases: The main transmission path is long-residence-time aerosol particles (< 2.5 μm), which are too fine to be blocked, and the minimum-infective dose is smaller than one aerosol particle.
The present paper about masks illustrates the degree to which governments, the mainstream media, and institutional propagandists can decide to operate in a science vacuum, or select only incomplete science that serves their interests. Such recklessness is also certainly the case with the current global lockdown of over 1 billion people, an unprecedented experiment in medical and political history.
Review of the Medical Literature
Masks and respirators do not work.
There have been extensive randomized controlled trial (RCT) studies, and meta-analysis reviews of RCT studies, which all show that masks and respirators do not work to prevent respiratory influenza-like illnesses, or respiratory illnesses believed to be transmitted by droplets and aerosol particles.
Furthermore, the relevant known physics and biology, which I review, are such that masks and respirators should not work. It would be a paradox if masks and respirators worked, given what we know about viral respiratory diseases: The main transmission path is long-residence-time aerosol particles (< 2.5 μm), which are too fine to be blocked, and the minimum-infective dose is smaller than one aerosol particle.
The present paper about masks illustrates the degree to which governments, the mainstream media, and institutional propagandists can decide to operate in a science vacuum, or select only incomplete science that serves their interests. Such recklessness is also certainly the case with the current global lockdown of over 1 billion people, an unprecedented experiment in medical and political history.
Review of the Medical Literature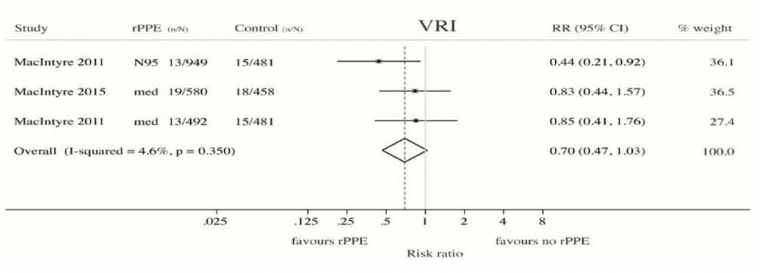

 Download Issue : Infection Control Today, June 2020 (Vol. 24 No. 5)
Download Issue : Infection Control Today, June 2020 (Vol. 24 No. 5)




